442 visitors from Jan 2013
International collaborative group aiming to create, support and disseminate research in cardiovascular field providing CRF web-based platforms for multicenter studies
Coordinator and creator: Enrico Cerrato; Fabrizio D'Ascenzo
Scientific Board: G.Biondi-Zoccai; J.Escaned; C.Moretti; G.Campo; I.Sheiban; C.Templin; I.Nuñez-Gil; S.Raposeiras Roubín; W.Wojciech; L.Perl; F.Varbella
Injeneering: D.Gallo; U.Morbiducci
Read News
Dabigatran versus Warfarin in Patients with Mechanical Heart Valves: the RE-ALIGN trial – Dr. I.Meynet
The oral direct thrombin inhibitor dabigatran has proven efficacy in preventing
thrombosis in patients with atrial fibrillation (RE-LY study), but its role
as an alternative to warfarin in patients with prosthetic valves is still unclear.
RE-ALIGN was a prospective, randomized, phase 2, open label trial with
the aim to validate the use and the dosing of dabigatran in patients with mechanical
heart valves.
Patients undergoing implantation of a mechanical bileaflet valve in the aortic
or mitral position or both (population A), or carriers of a mechanical bileaflet
mitral valve from more than 3 months (population B), were enrolled from November
2011 in 39 centers worldwide. All included patients were randomized to receive
dabigatran or warfarin in a ratio of 2:1; the starting dose of dabigatran was
targeted on the basis of renal function (150, 220 or 300 mg twice-a-day), and
the following dose was adjusted in order to obtain a plasma level of dabigatran
of 50 mg/ml or higher; the dose of warfarin was adjusted to obtain an international
normalized ratio (INR) of 2 to 3.5, according to the risk profile of each patient.
After 12 weeks of treatment, patients in the dabigatran group could choose to
switch to warfarin or to continue. The study was discontinued after 12 months
due to excess thromboembolic and bleeding events among the dabigatran group.
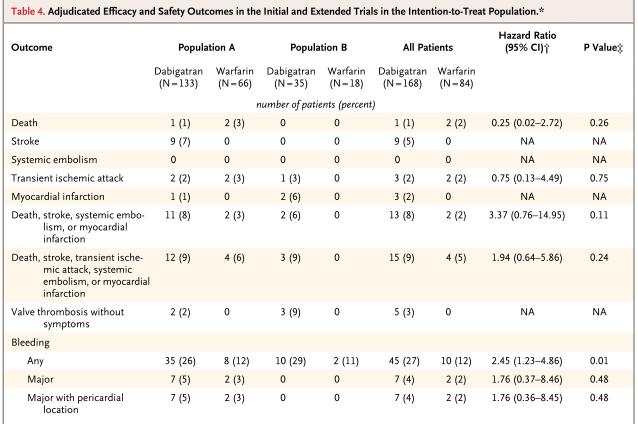
5 out of the 252 enrolled patients experienced valve thrombosis, 9 had stroke
and 3 had myocardial infarction, all in the dabigatran group; a major bleeding
episode occurred in 7 patients in the dabigatran group and in 2 patients in
the warfarin group (HR 2.45, p = 0.01), and all of them were pericardial bleeding
(see table). Patients in the dabigatran group reached the targeted plasma level
of 50 ng/ml for an average of 86% of the time, and dose adjustment or discontinuation
of the drug was required in 52 of 162 patients (32%).
Warfarin may be more effective because it inhibits both the coagulation pathways
as well as the common thrombin pathway, while dabigatran exclusively inhibits
thrombin. In the setting of patients with prosthetic valves, the triggers for
the formation of thrombi are probably more complex and stronger (including the
exposure of the blood to the artificial surface of the valve and the damage
of tissues during surgery) than in patients with atrial fibrillation (in whom
thrombi form in low-flow, low-shear, low-stress conditions in the left atrial
appendage). Taken together, those two reasons may explain the lack of protection
from thrombosis with dabigatran. Dabigatran is therefore not appropriate
as an alternative to warfarin in patients who require anticoagulation after
the implant of a prosthetic valve, showing no benefit and being associated with
an increased risk of bleeding. N
Engl J Med. 2013 Sep 26;369(13):1206-14.
writed at 20-10-2013 23:01:29